
Client Intake Form
Contact Information
Name___________________________________________________
Date______________________________
Address_____________________________________ City________________________ State_________ Zip______
Phone(home/work/cell)______________________________________________________________
E-mail____________________________________________
Birth Date_______/_______/__________
Emergency Contact__________________________________________
Relationship____________________________
Phone(home/work/cell)______________________________________________________________
How did you hear about us?________________________________________________________________
Current Health
Have you ever received massage therapy before? Y N
When/Results_______________________
How are you feeling today? ______________________________________________________________
Reason for today’s visit ________________________________________________________________
Please indicate areas of your body to pay special attention to______________________________
Please indicate any areas of your body you do not want touched____________________________
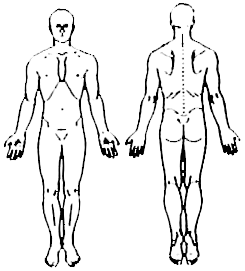
Please use the diagram below to indicate areas of tension or discomfort
Medical History
Occupation/Activities/Hobbies_________________________________________________________
Are you currently under the care of a physician? Y N
Name, phone number, and what for__________________________________________
Are you taking any medications or other substances (supplements, herbs, alcohol, or recreational drugs)?__________________________________________________________________________
Please list any surgeries, accidents, or major illnesses_______________________________________
Have you ever been diagnosed with cancer? Y N
Type and current condition______________________________________________________
Do you have any communicable diseases? Y N
Type and current condition____________________________________________________
Consent for Care
It is my choice to receive massage therapy. I am aware of the benefits and risks or massage and give my consent for massage. I understand that there is no implied or stated guarantee of success or effectiveness of individual techniques or series of appointments. I acknowledge that massage therapy is not a substitute for medical care, medical examinations, or diagnosis. I have stated all medical conditions that I am aware of and will inform my practitioner of any changes in my health status.
Client Signature__________________________________________________
Date____________________

 Dana Davis is the massage therapist and sole proprietor of Midnight Sun Massage. The focus of Dana’s practice is to facilitate the body’s natural healing abilities in clients suffering from chronic pain, injuries, illness, and stress.
Dana Davis is the massage therapist and sole proprietor of Midnight Sun Massage. The focus of Dana’s practice is to facilitate the body’s natural healing abilities in clients suffering from chronic pain, injuries, illness, and stress.